Share Post
How can puppetry and robotics help us to better understand the place of simulation in clinical education?
War Horse tells the moving story of Joey, a horse taken from rural Devon to the morass of Flanders during the First World War. A fundamental challenge for the stage adaptation was bringing Joey to life within the confines of a theatre. Seen at rest, the puppet created by Handspring has a superficial resemblance to a horse but remains a crude, fabricated representation.
The Puppetry brings galloping, full-scale horses to life on stage—their flanks, hides and sinews built of steel, leather and aircraft cables.
Handspring
There has been no attempt to hide the strings. The genius of the puppetry is in its focus on the essence of being a horse: as Joey starts to move, his ears go back, his flank twitches and his tail flicks. As he starts to trot and then canter round the stage the three, very visible puppeteers fade away. And as he becomes heart wrenchingly caught in the barbed wire, I certainly wasn’t the only grown man in the audience who was crying.
A similar challenge is faced in medical simulation: how do you bring a mannequin, or a part task trainer to life in a simulation suite? The key focus for many developers and users of simulators over the last thirty years, has been the concept of fidelity. The relevant dictionary definition of this word is resemblance and simulators have been classified as high or low fidelity depending on how much they look, or feel, or sound like the real thing.
The ideal example… would be the Star Trek ‘‘holodeck’’, in which one literally cannot tell the difference between the simulated experience and real life.
David Gaba
The premise has been: the closer the approximation, the better the student will learn, the ultimate goal being simulation that is indistinguishable from real life. In this post I’ve tried to unpick some of the thinking behind these assumptions.
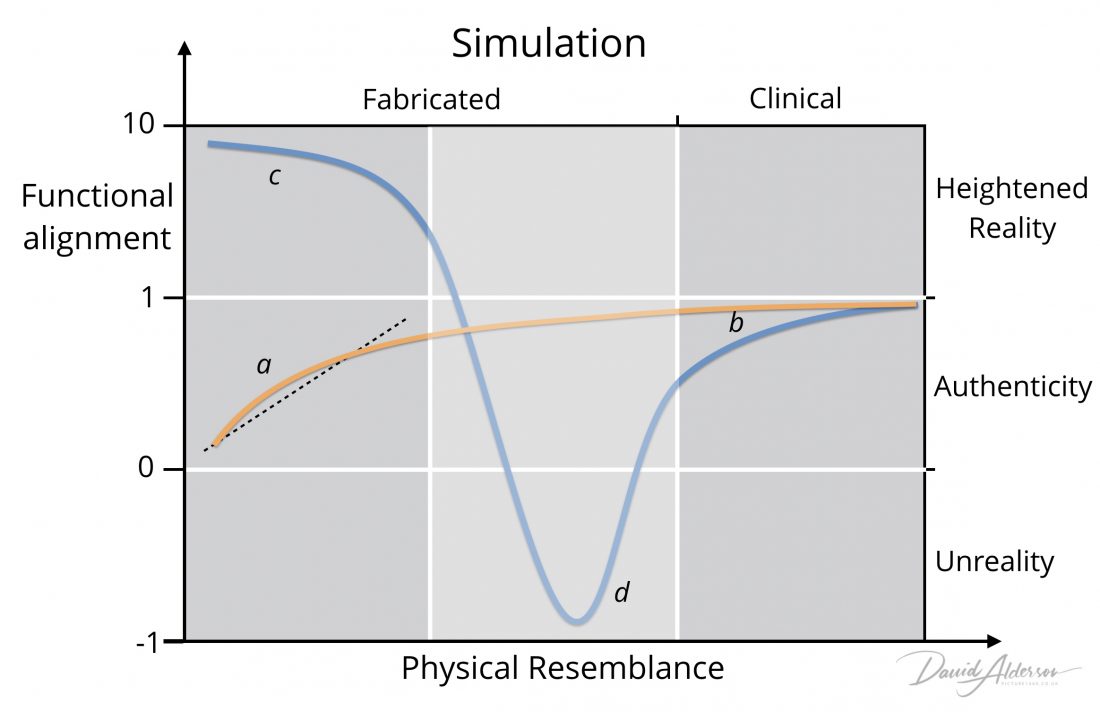
When we are considering whether something is true to life we need to think in (at least) two dimensions. Stanley Hamstra and others have argued that, as a minimum, both physical resemblance and functional alignment should be considered. Take a look at the diagram at the top of the page: the brown line represents an orthodox understanding of simulators. It shows a dependent relationship between these variables of form and function: the more a simulator resembles the patient, the greater the alignment, and the more a student will learn.
High fidelity mannequins try to represent a patient using precise modelling, soft skins, opening eyes and accurate body sounds. Technicians add wigs, make up, clothes and wounds, aiming to more closely reflect our physical perceptions of a clinical scenario. On the left (box a) we see that the brown line deviates from a linear relationship: there is an acknowledgement that high fidelity simulators may over-promise and that some, perhaps peripheral aspects of clinical care may be missing. Conversely, low fidelity simulators may prove of some value educationally despite their obvious limitations.
I remember the first time I gave an injection: the first time I had penetrated another person’s skin with a sharp instrument. Practicing the actions on an orange made a great deal of difference, although it still took considerable courage to overcome the cultural and innate taboos of violating another living human body.
All too often it is the surface realism of the simulation that occupies the ingenuity of those who develop it, eclipsing key issues of teaching and learning
Roger Kneebone
The orthodox assumption has been that the orange is always going to be second best to a higher fidelity simulator. So companies fabricate and market models that look like an arm, and feel like real skin and muscle, in a never-ending search for authenticity. There is always a trade off with cost, of course, but the presumption remains that higher fidelity means better.
At the far right of the figure we can see where these conventional aspirations of simulation—practice indistinguishable from real life—have already been achieved (box b). When I have a junior registrar with me in the operating theatre, I choose which sections of which operations they should perform. I set up the conditions to make things go smoothly. I take responsibility for the time pressures and ultimately for the clinical outcomes. I create a clinical simulation of my role as a surgeon. As the registrar progresses these supports fade, but they are always present. The danger arises when the registrar does not realise that they are still performing within a simulation, leading to hubris and the potential for a fall when they make the large step to becoming an independent consultant surgeon. While the brown line represents orthodox understanding, the blue line shows the actual situation. It is important to ensure that my trainees recognise this authenticity gap.
Following the blue line back to the left of the figure, the inherent desirability of higher fidelity in fabricated simulation is also challenged (box c). Our perspective on simulation changes to one of re-imagining clinical practice, as a heightened reality that can enhance learning beyond any authentic re-creation: even better than the real thing. Portraying a functional essence of Joey, at the expense of physical resemblance, resonates strongly with audiences. Perhaps attaching an orange to a real person’s arm provides a better simulation of the act of transgressing another’s body with a steel needle than a fabricated arm could ever do.
The prosthetic hand has achieved a degree of resemblance to the human form…however, when we realize the hand, which at first sight looked real, is in fact artificial, we experience an eerie sensation…we lose our sense of affinity, and the hand becomes uncanny.
Masahiro Mori
The field of robotics and puppetry provides a further warning about the dangers of chasing fidelity towards every closer resemblance. Masahiro Mori identified that giving robots human-like appearances creates a stronger emotional connection—up to a point. As the robots start to approximate humans, they begin to evoke feelings of disgust and revulsion: a concept popularised as the uncanny valley.
In simulation, there is a risk that the attempt to fabricate ever closer replicas will lead both students and teachers to believe that the holodeck they are jointly exploring is truly authentic, while they are actually mired in the depths of unreality (box d). The professional-artistry of clinical care cannot be reduced to technical-rational reconstructions: vital aspects of that practice will be invisibly, but invariably, absent. If we are not careful, an overriding focus on the five physical senses may miss the intuitive, sixth sense of insight, foresight and gut feeling; the ethical sense of decency, and right and wrong; the poised sense of balance and perspective; emotional sensitivity and common sensibility. Learning through simulation may become an uncanny dissimulation of clinical learning.